
Kangubator
An industrial design project to develop a low-cost disposable sling supporting Kangaroo Mother Care for vulnerable newborns in transport and NICU settings.
Problem Summary
In India, many low birth weight (LBW) and premature newborns born in resource-limited centers require transportation to higher-level facilities. However, poor neonatal transport conditions and lack of critical equipment such as incubators lead to increased mortality rates for transported newborns due to Noise & Vibration (NV) stress, hypothermia, and other factors. With over 60% of LBW births occurring in hospitals with limited neonatal care, a significant number of neonates rely on unreliable transport options like motorbikes or auto-rickshaws, without proper stabilization. Improving transport conditions is essential to reduce neonatal mortality in India.
Project Brief
How might we reduce mortality and morbidity among low birth weight and premature newborns during transport in resource-limited settings in India?
Research
Our research began with in-depth desk research, online ethnography, and observations through videos and medical forums, providing a strong foundation on neonatal healthcare and transportation.
We then conducted field research, interviewing users and experts, and engaging in activities like guerrilla observations and shadowing healthcare professionals in Karnataka and Telangana. These methods gave us real-world insights, which we used to create mind maps and user journey maps for a clearer understanding of neonatal transport and its risks.
The fieldwork was done in two phases: Phase 1 focused on urban healthcare settings, and Phase 2 on rural healthcare settings. Comparing both phases highlighted how geography, infrastructure, and access significantly impact neonatal transportation and the healthcare system.
40+ healthcare professional Interviews conducted, 9 healthcare facilities across 4 districts (In urban and rural areas), 20+ rural healthcare center patients interviewed
Primary Research: In-depth desk research (Patents, healthcare studies, articles and statistical reports), online ethnography and observations
Field Research: User & expert interviews, guerrilla observations, shadowing healthcare professionals, mind map and journey maps.
Phase 1: Urban Healthcare
Public Hospital Challenges: At Niloufer Hospital in Hyderabad, one of the region’s largest public hospitals, we observed the strain of high patient volumes, limited resources, and fast-paced decision-making. Despite these challenges, staff adapted to maintain care quality.
Private Hospital Advantages: In contrast, private institutions like Avis Ankura Hospital and St. John’s Medical College offered more stable environments with better staff-to-patient ratios and efficient systems. These conditions enabled more personalized and preventive care, highlighting the impact of strong operational management.
Diverse Perspectives: Interviews with 20+ healthcare professionals, including private clinic doctors, revealed wide variations in neonatal transport and referral practices, influenced by institutional capacity, workload, and infrastructure





Public hospitals faced resource strain and high pressure, while private ones offered stability and better staffing with similar equiment quality.
Medical professionals’ views and perspectives are strongly shaped by the institutional environments in which they work.
Phase 2: Rural Healthcare
Building on Phase 1, we conducted fieldwork in Karnataka’s Koppal and Shimoga districts, covering towns and villages. With limited private healthcare, the focus was on public facilities like Primary Health Centers (PHCs), Community Health Centers (CHCs), and Sub-Centers. Interviews and observations with 15+ healthcare professionals revealed clear contrasts with urban healthcare.
Infrastructure Gaps: Rural facilities faced severe shortages in infrastructure, equipment, trained staff, and consistent services. Many lacked essential resources like ambulances or specialist doctors, limiting emergency care.
Low Awareness and Dependence: Patients and families showed low awareness of health services and preventive programs. Due to limited literacy, many relied heavily on local doctors and ASHA workers for health decisions, exposing gaps in outreach.
Transport Challenges: Emergency neonatal transport was scarce or nonexistent. Families often depended on personal vehicles or irregular public transport, causing delays that increased risks in critical maternal and neonatal cases.




There is a lack of healthcare infrastructure and resources, coupled with low awareness of available services and programs.
Due to low literacy, people in rural areas often depend on healthcare professionals for final guidance.
Social Healthcare Professionals:
We had the valuable opportunity to meet and interact with ASHA health workers during our time in Koppal. Accredited Social Health Activists (ASHAs) are government-appointed community health workers who play a key role in rural healthcare. They serve as a vital link between the community and the public health system, focusing on maternal and child health, health education, and disease surveillance.
ASHAs are well-respected in rural areas and often serve as the first contact for those seeking medical help, especially when transport to higher-level facilities is needed. Due to limited formal transport in many rural regions, ASHAs often depend on volunteer-based support from neighbouring villagers.

ASHA workers mainly rely on volunteer-based support for emergency situations.
Insights
"We often see babies arrive hypothermic because of prolonged transfers and no proper warming devices and transport."
Neonatologist, Niloufer Hospital, Hyderabad
"We do not have ambulances designed specifically for neonates. We manage with what is available and improvise."
Pediatrician, Primary Health Centers (PHCs), Koppal
"Training paramedics and nurses in neonatal care during transport is as crucial as having good equipment."
Senior Neonatologist, Bangalore
Market Study:
Cloth Wraps & Slings

No heating element
Cost-effective
User-friendly and easy to clean
Appropriate for stable, healthy newborns
Widely used for covering and transporting infants
Compatible with all modes of transport
Heated Carriers & Slings

External heating element
Moderately priced
More complex to use and clean compared to cloth wraps
Designed for preterm and low birth weight infants
Compatible with all modes of transport
Provides effective thermoregulation
Incubators & Warmers

Ideal method of transporting sick infants
High cost
Requires trained healthcare professionals for use
Suitable for critically sick infants
Usable only in select ambulances
Synthesis
Based on the information collected through our research activities, we created a roadmap on how neonatal transport occurs currently and highlighted parts in organge where infants face the most amount of danger.

Equipment Required During Transport
Equipment attached to neonate:

Only a single piece of equipment tubing is connected to one limb.
Essential Equipment Recommended for Safe Neonatal Transport:
Transport incubator or portable infant warmer
Neonatal transport ventilator (or bag-valve-mask system sized for neonates)
Cardiorespiratory monitor (for heart rate, oxygen saturation, respiratory rate)
Infusion pumps and syringe drivers (for IV medications and fluids)
Oxygen cylinder with flowmeter
Suction device
Thermal blankets or portable warming devices
Emergency drugs and neonatal resuscitation kit
Currently Available in Most Settings (Based on Field Observations):
Basic oxygen cylinder (often without neonatal flow adjustments)
Manual resuscitation bag (variable availability)
Makeshift warming methods (hot water bottles, kangaroo care)
Limited or no monitoring devices (vitals often not tracked in transit)
Infrequent access to transport incubators (usually absent in smaller hospitals)
"We often only have oxygen and a bag & mask with us. No monitors or warmers."
Pediatrician, Primary Health Centers (PHCs), Shimoga
Neonatal Transport: Relevant Statistics

39% of admissions in the NICU are outborn neonates
Outborn infants :
The infant was delivered at one healthcare facility but transferred to another for treatment.
Inborn infants :
The infant was both delivered and treated within the same healthcare facility.

Birth Weight:
Infants under 2500 g of weight are classified as Low Birth Weight infants (LBW).
58% outborn infants are LBW.


Gestation Period:
Infants born >34 weeks of gestation are classified as premature.
51% of outborn infants are premature born.


Society sectors:
73% of infants admitted to the NICU come from underprivileged segments of Indian society.
Infant Mortality & Diseases and Disorders in Outborn Infants

Mortality is higher in outborn infants (15%) than in inborn infants (9%).
Common diseases & disorders in outborn infants
Jaundice
Congenital malformations
Birth-related complications
Respiratory distress syndrome
Sepsis
Pneumonia
Meningitis
Others
Reasons for higher mortality in outborns:
Inadequate pre-transport stabilization
Improper or insufficient care during transport (e.g., untrained staff, poor hygiene, exposure to external factors, limited caregiver awareness and skills)
Lack of proper monitoring en route
Limited or unsuitable medical equipment
Risk of clinical deterioration during transfer
Extended travel durations
Unsuitable or unsafe modes of transport
What is Clinical Deterioration?
Clinical deterioration in infants—marked by declining vital signs like temperature, heart rate, or oxygen levels—is especially dangerous for preterm or low birth weight babies due to their vulnerability. Preventing this during transport requires careful pre-transport stabilization, including thermal regulation, airway management, and maintaining oxygen and glucose levels. Continuous monitoring, attentive care, trained personnel, proper equipment, and safe transport conditions are all essential to ensure infant stability throughout the journey.
Infant Stabilization Before Transport
Assess the infant’s condition, including vital signs and physical exam, and address urgent medical needs before transport.
Ensure stability by focusing on TOPS: Temperature, Oxygen, Blood Pressure, and Sugar.
Stabilization may take 15–60 minutes, depending on severity.
Manage common issues like hypothermia, hypoglycemia, poor perfusion, and respiratory distress.
Serious risk for infants during transport. Stabilization and monitoring by trained personnel with appropriate equipment critical to maintaining stability.
A low-cost way to to avoid Clinical Deterioration during transport?
During our fieldwork in India, we engaged with over 50 healthcare professionals and identified a strong need for effective thermoregulation during neonatal transport in low-resource settings. Kangaroo Mother Care (KMC) emerged as a practical solution.
KMC, or skin-to-skin contact, involves placing a premature or low birth weight newborn chest-to-chest with a parent to maintain warmth and support breastfeeding. It helps prevent hypothermia, especially at home without equipment or access to advanced care.
Endorsed by the WHO, KMC is a proven alternative to incubators, suitable for hospitals, NICUs, homes, and transport.
In rural districts like Koppal and Shimoga, KMC is widely promoted. We saw many informational boards outlining its benefits, reflecting its growing role in community healthcare.
What is Kangaroo Mother Care?
Reduces morbidity and mortality in preterm and low-birth-weight infants
Reduces pain in infants
Promotes breastfeeding
Improves bonding with parents and parental confidence
Reduces load and dependency on health institutions
Benefits of Kangaroo Mother Care?

KMC, endorsed by WHO, uses skin-to-skin (chest-to-chest) contact to prevent hypothermia and support newborns in low-resource settings.
Insights regarding Kangaroo Mother Care:
"KMC is helpful during transport when done right, but caregivers often don’t feel confident or are not guided properly.
You transport the baby in the condition in which transport was initiated. That’s where thermal care like KMC makes a difference."
Neonatologist, St. John’s Hospital, Bangalore
"KMC alone is not enough in longer transports. We need reliable warming support devices as well."
Pediatrician, Private Hospital, Bangalore
"KMC is better than nothing. If there's no equipment, the mother’s body is the incubator."
Neonatologist, Avis Ankura Hospital, Hyderabad
Project Brief
How might we reduce mortality and morbidity among low birth weight and premature newborns during transport in resource-limited settings in India?

Rephrased Project Brief
How might we make Kangaroo Mother Care (KMC) a safe, practical, and culturally acceptable method for newborn transport in low-resource settings in India?
Design & Prototyping
Based on our research, key takeaways, and revised project brief, we developed design criteria that formed the foundation for our design process. We applied these criteria to the frame of an existing sling created by Bempu Healthcare. This led to the development of 8+ concepts for the Kangubator, with 100+ iterations and multiple rounds of in-house testing.
This process resulted in the final prototype, which was taken for clinical testing at Niloufer Hospital in Hyderabad, India.
Below are images of the various prototypes.







Kangubator
Final Concept
The Kangubator is a low-cost, disposable wearable sling designed to support Kangaroo Care during the transport of low birth weight and preterm infants. Acting as a human incubator, it helps prevent hypothermia, neurovascular stress, and related complications. It ensures essential skin-to-skin contact while providing adequate coverage for the caregiver, and simulates in-utero conditions to promote infant stability. The Kangubator is reusable during both transport and NICU care until the infant’s condition stabilizes.
Design Criteria
Unisex and one-size-fits-all design for universal caregiver compatibility
Ergonomically designed for safe and comfortable placement of the neonate
Made from infant-safe, compatible materials
Allows for easy visual monitoring of the neonate during transport
Washable and reusable
Supports integration with medical equipment such as syringe pumps, feeding aids, vital sign monitors, and respiratory support devices

Design Features
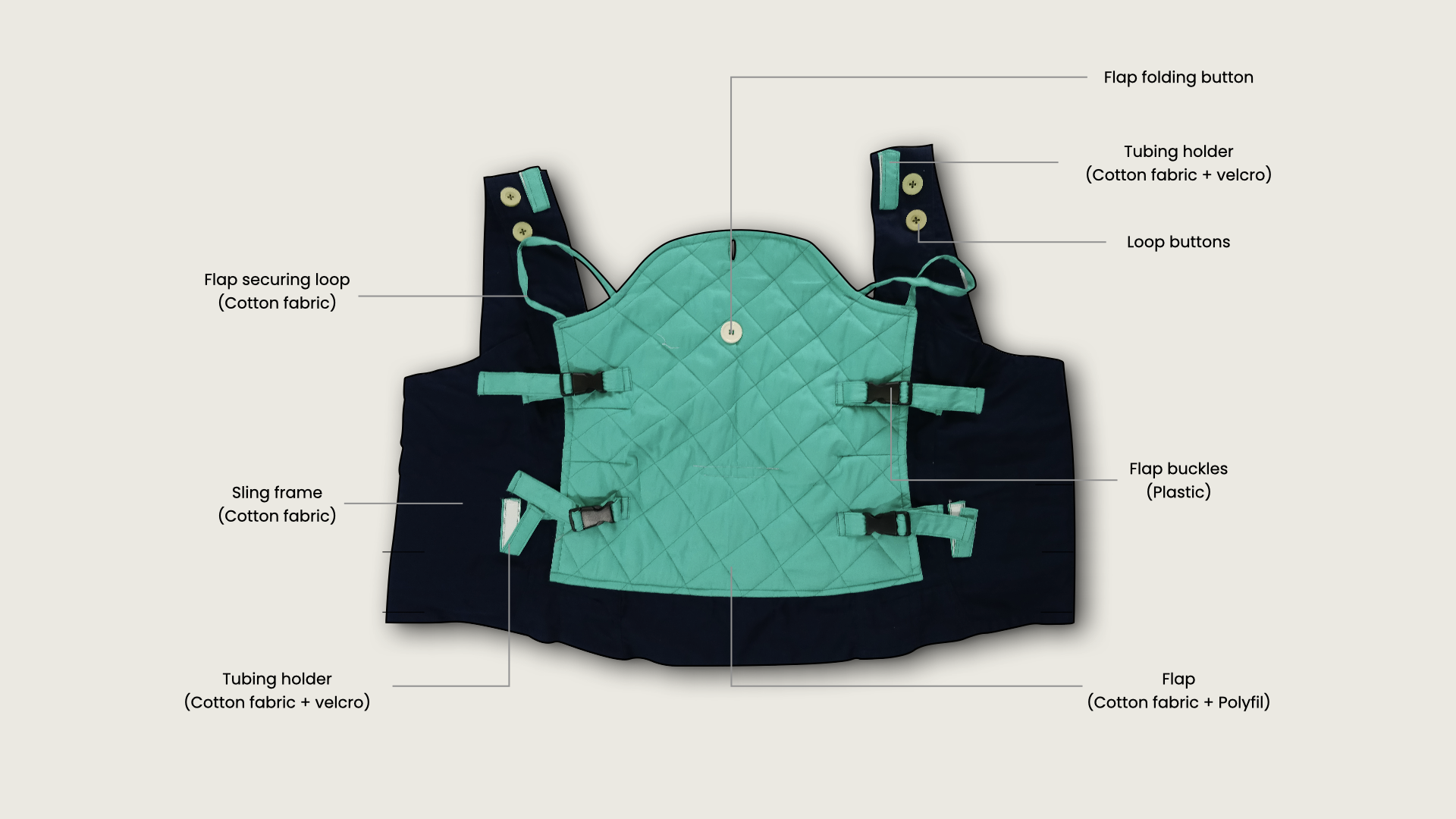



The Kangubator prototypes were assessed in-house at Bmpu Healthcare, testing fit and dimensions with employees of diverse heights and body types.







How to wear Kangubator?

How to attach tubing?

Clincal Testing & Validation
Between December 2019 and March 2020, the Kangubator was evaluated with 65 sick or premature infants and their parents practicing Kangaroo Mother Care (KMC) in the NICU at Niloufer Hospital, a government-run neonatal facility in Hyderabad, India. While clinical testing in the NICU was successful, hospital approval for testing in a transport setting was not granted, leaving that area untested.
Most parents reported no difficulties or anxieties using the Kangubator. Of the 65 participants, 56 parents found it comfortable for KMC, even with babies connected to medical equipment like CPAP machines.
Infant weight gain and breastfeeding comfort were monitored as key indicators. Results showed 47 infants gained weight steadily, and 50 mothers reported improved comfort and bonding during breastfeeding.
Tested with 65 sick or premature infants and their parents in a NICU setting.
Hospital approval for testing in a transport setting was not obtained, so no transportation testing data is available.
56 parents found it comfortable with equipment, 47 infants gained weight steadily, and 50 mothers reported better breastfeeding comfort and bonding.








View more case studies.